Infection control is everybody's business
“Nosocomial infections are still a major issue and require continued attention,” says Sophie Baillargeon, MUHC interim associate director of Nursing (ADON) for Quality, Performance and Patient Engagement. “We know that proper hand hygiene is the most effective infection control measure. Yet, we don’t wash our hands often enough or disinfect the equipment and the environment as much as we should and when we should. The Controlling Specific Infection - Successful Strategies (CSISS) program was developed to change that situation.”
Since March, four teams at the Glen site of the McGill University Health Centre (MUHC) – Units B9 (Departments of Pediatrics), C9-D9 (Department of Internal Medicine) and the Transport service – have been implementing a series of successful strategies within the CSISS program to improve hand hygiene (HH), environment cleaning and disinfection.
Champions to spread the message
The CSISS program begins with education. Members of each team receive training and some of them, like transport attendant Joshua Pinto, become champions. Joshua is responsible for reinforcing the message that infection control is everybody’s business.
“I did a couple of training sessions about proper hand hygiene, glove use and equipment cleaning,” says Joshua, who has frequent direct contact with patients. “Now, I answer my colleagues’ questions, and if someone is not following the proper procedure, I will remind them nicely of what to do.”

“People need to be kept up to date, or else bad habits start to form. We’re trying to educate the team and develop a different type of culture where everybody is on the same page. The message is to wash your hands and equipment properly and to not use gloves when you don’t need to. If we follow these steps, we can eliminate nosocomial infections. Our goal at the MUHC is zero infections.”
According to Anaïck Briand, project manager for the Nursing Improvement Program, training has produced excellent results in the Transport team.
“Before the training, they would wash hands 93 per cent of the time when entering a patient’s room and only 55 per cent when exiting. After the training, they washed their hands 96 per cent of the time both coming in and out of a room. Proper glove use has also improved significantly.”
Audits to monitor hand-washing
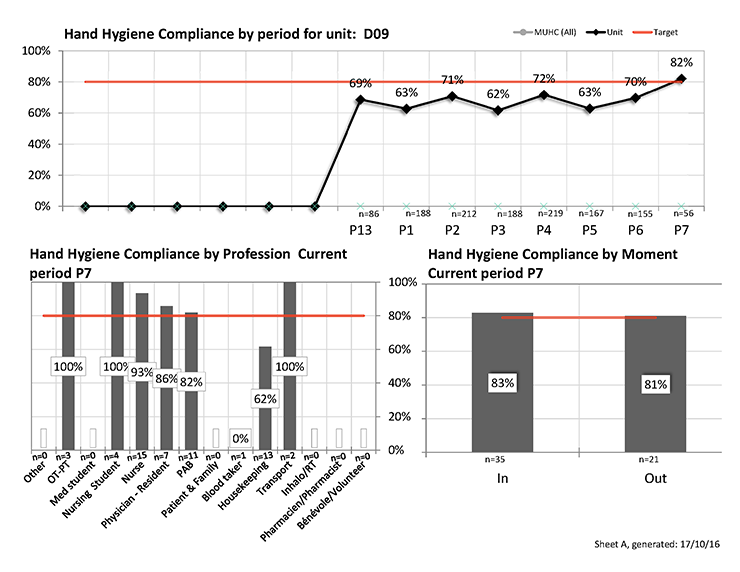
The Nursing Leadership team, as well as the Infection Control Practitioners, have been performing frequent audits on the teams. On C9 and D9, every member of the healthcare team, including patient attendants, housekeepers, nurses, nursing students, residents and physicians, are monitored for their HH and disinfection practices.
“We use electronic tablets and two types of software to record data about hand hygiene as well as routine cleaning practices, discharge cleaning, and proper use of protective gear (gloves, gowns , etc.),” says Aparna Bhattacharjee, nurse manager of C9-D9 Internal Medicine. “The Quality Management department then compiles the results and produces graphs that reflect our reality. This technology, and the data it produces, has taken the discussion of hand hygiene from an abstract concept to personalized, tangible data that can be discussed with our team as well as with our housekeeping and physician colleagues. Thanks to our audits, hand-washing among the nursing team, physicians, and housekeeping has improved dramatically.”
Huddles to keep everybody on the same page
One important element of the CSISS project is the weekly huddle, a moment where members of the team and the infection control practitioner gather in front of the quality station whiteboard to review objectives, assess infection rates and analyze results of the hand hygiene observation audits.

The meetings have become a habit for the teams, a moment to celebrate little victories or to face problematic situations head on.
“The huddles are extremely important,” says Aparna. “We invite every member of the healthcare team to meet for 15 minutes to review information on the latest audits and results, and new incidences of nosocomial infections. If everything is going well, we cheer each other on. If there’s a problem, it will be resolved.”
According to Aparna, the key to the success of the project is that “it draws on the strength and commitment of the wonderful individuals who work in the unit. We encourage and welcome ideas from everyone. For example, one day during a huddle we were discussing a C. difficile outbreak (Clostridium difficile), when one of our PABs, Jean-Claude Cadeau, said, ‘Oh, what about the stations with wipes outside each room? They are hydrogen peroxide wipes. Maybe we should change those containers for the bleach wipes during an outbreak?’ That was an excellent idea, and we adopted it.”
Empowering staff
Tom Lombardi, section manager for Patient Transport, also sees benefits in empowering caregivers.
“We receive reports of the situation on each site every week. During the huddles, we write down ideas and the name of the person who came up with them. They feel like they’re being heard.”
For Anaïck and her colleagues, it was important to try different strategies with the teams and see what works.
“We work consistently, taking small steps,” she says. “We can adopt, adapt or abandon an idea, without investing a lot of money, time or resources. Most importantly, this project makes us aware of the impact our actions can have on the rates of nosocomial infections and, consequently, on the health of our patients.”
Encouraging results
According to Dr. Caroline Quach, pediatric infectious diseases and medical microbiologist and co-director of the MUHC Vaccine Study Centre of the Montreal Children’s Hospital (MCH-MUHC), staff at the MCH was already aware of the importance of infection prevention and control, with champions for each service and unit and regular hand hygiene auditing. Yet, there were still cases of healthcare-associated viral respiratory tract infections, even if multi-drug resistant organisms had not been transmitted.
“The CSISS piloted on B9 brought on quality improvement methods, and it has been amazing to see that, with the involvement of an entire team in the CSISS pilot project, there has been a marked decrease in transmission of upper respiratory infections. It is too early to tell if this will be sustained throughout the next winter season, but it is a good start and is quite encouraging!”
“The outcomes obtained by the program have been just phenomenal,” says Dr. Charles Frenette, MUHC medical director of Infection Control, noting that the units involved have almost eradicated acquisition of C. difficile and VRE (vancomycin-resistant Enterococcus faecalis), and transmission of MRSA (methicillin-resistant Staphylococcus aureus).
“This is something we would have never thought possible two years ago,” he says. “Thanks to this program not only are we making our environment safer for our patients, but we are also saving costs to the hospital so that our limited resources can be better used.”